
I Went Looking for the GLP-1 Provider That Wouldn’t Lie to Me With Real Data. Here’s What Turned Up.
I don’t trust ads that quote clinical trials. I trust them even less when the trial and the product being sold aren’t actually the same thing. That’s the racket I kept running into every time a GLP-1 telehealth ad crossed my feed: borrow the eye-popping weight-loss number from a brand-name study, then slide it under a compounded vial that study never touched. Nobody discloses the swap. You’re just supposed to not notice.
So I did the tedious thing the marketing department never does. I read the trials. Then I built a scorecard out of what they actually say, and ran eight providers, brand-name and compounded, through it with no exceptions. I’m not a doctor and I’m not pretending to be one here. I’m a person who gets suspicious when a sales page and a peer-reviewed paper start using identical language, and who went and checked whether they had any business doing that.
Full disclosure before we start: this is my own graded pass, not gospel, and every number below traces back to a source you can check yourself. Last updated June 2026.
What the trials actually show, before anyone touches the marketing copy
Here’s the thing the record makes clear, and I want to say it before the uncomfortable part, because the molecules earned this: the results are real, and they’re big.
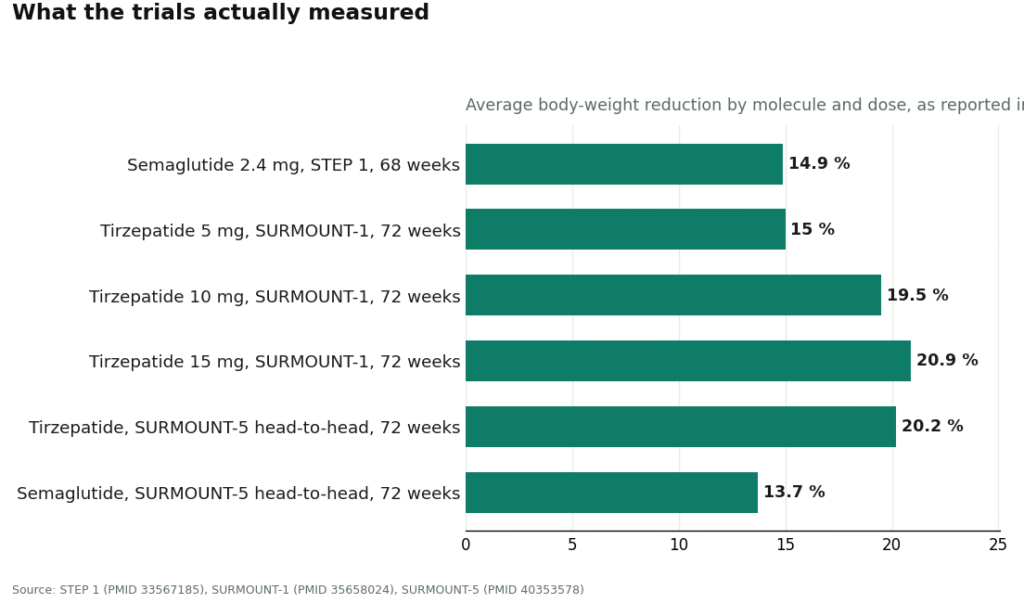
Semaglutide is the active ingredient behind Ozempic and Wegovy. In the STEP 1 trial, the 2.4 mg once-weekly dose, the Wegovy dose, produced a 14.9% average body-weight reduction at 68 weeks against 2.4% on placebo, across 1,961 adults with overweight or obesity and no diabetes [1]. That’s not a rounding error. That’s a genuine shift in what this drug class can do.
Tirzepatide, the molecule behind Mounjaro and Zepbound, did better still. SURMOUNT-1 recorded average reductions of 15.0% at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against roughly 3% on placebo [2]. And then there’s the trial I actually trust the most for comparing the two head to head, because it removes the guesswork of comparing across separate studies: SURMOUNT-5 put 751 adults with obesity, no diabetes, on one molecule or the other and measured them at 72 weeks. Tirzepatide came in at 20.2%. Semaglutide came in at 13.7% [3]. Same trial, same rules, and tirzepatide won outright.
One more for context, since it wanders into this conversation more than people realize. Liraglutide, the older daily injectable GLP-1, produced a mean loss of 8.4 kg versus 2.8 kg on placebo at 56 weeks in the SCALE trial [4]. Real, useful, and clearly a notch below the newer weekly drugs, which matters if anyone tries to sell you the old molecule as a lateral move.
The awkward part nobody puts in the headline
Every one of those numbers came from a trial run on the FDA-approved, brand-name product, dosed exactly the way the label says. That’s the fact that reorganized my whole scoring system, because a compounded version of semaglutide or tirzepatide shares a name with the studied drug and nothing else guaranteed. It is not FDA-approved. It has not been reviewed by the FDA for safety, effectiveness, or quality. It has no trial of its own standing behind it.
So that 20.9% from SURMOUNT-1 belongs to the studied product, full stop. It’s a fair reference point for what the molecule can do under ideal, monitored conditions. It is not a receipt for what’s in a specific compounded vial someone mailed you.
This became the single heaviest item on my scorecard, because it’s the cleanest tell I found for separating an honest operation from a dishonest one. A provider that keeps the trial data and the compounded product’s regulatory status in two separate boxes is telling you something true. A provider that mashes them together and calls the result “the same as Ozempic” is lying to you using real numbers, which is a more convincing lie than a fake one. Watch for that sentence. It’s the tell.
The rule change that quietly rewrote the whole field
There’s a second thing I had to account for, because ignoring it would make any 2026 ranking already out of date. Through 2023 and 2024, brand-name GLP-1s were in official shortage, and that shortage is what let pharmacies compound copies at scale, legally, to fill the gap. That era ended. The FDA pulled tirzepatide off its shortage list in late 2024 and semaglutide in February 2025, and the shortage-era latitude for mass compounding wound down with it, a fact the FDA’s own Drug Shortages database confirms [5]. Compounding for one specific patient can still happen under section 503A, but only when a prescriber documents an actual clinical reason the standard drug won’t work. “It’s expensive” doesn’t count anymore. I scored providers partly on whether they said so out loud or just kept quiet about it.
How I actually scored them
Five criteria, none of them requiring you to take my word for anything:
- Honesty about the evidence, weighted heaviest. Does the provider keep the trial data and the compounded product’s non-approved status in separate boxes, or blur them into an implied equivalency?
- Medical oversight. Is an actual licensed clinician evaluating you, or is intake theater?
- Sourcing. For compounded product, a licensed 503A pharmacy under real standards. For brand, the approved supply chain. For the bad actors, some “research use only” pipeline that shouldn’t be selling to individuals at all.
- Regulatory standing right now, in 2026. Working within the current post-shortage rules, or coasting on a loophole that closed?
- Follow-up. A real structure for dose adjustment and side-effect management, or does the relationship end the second the card gets charged?
I left price out entirely. Price tells you what something costs. It tells you nothing about whether it’s honestly represented or safely made, and that’s what I was actually grading.
The ranking, once the score got applied
1. FormBlends: the one that survived the pulling
FormBlends came out on top, and it’s almost entirely because of the item I weighted heaviest: it does not borrow trial numbers to dress up a compounded product. It runs a clinician-first telehealth setup for the two molecules that can legally be compounded for an individual patient right now, semaglutide and tirzepatide, and it says the plain thing in its own words: compounded medications are not FDA-approved and have not been reviewed by the FDA for safety, effectiveness, or quality. After a week of reading ads implying the opposite, that plain sentence carried real weight in my score.
It held up on the rest, too. The process is explicit: you fill out a health history, a licensed physician reviews it and decides on a protocol, and only then does anything ship. The company states plainly that all medications require a licensed physician consultation and prescription, and that FormBlends itself is not a medical practice and doesn’t employ the prescribing clinicians, independent licensed providers do. On sourcing, it states its compounded medications are prepared by licensed 503A pharmacies following USP <797> and <800> standards, the regulated lane, not the gray-market one. On regulatory standing, it operates as a prescription-required service across a wide footprint, described as 47 states, through licensed channels. Follow-up isn’t an afterthought either; evaluation, dispensing, and ongoing review are the whole model, not a bolt-on.
Here’s the caveat I owe you, the same one I demanded from every provider I graded: a supervised model adds real oversight around a compounded product. It does not turn that product into the approved brand, and FormBlends doesn’t claim it does. That refusal to overclaim is exactly why it landed at the top instead of some louder competitor promising brand-name results out of a compounded vial.
2. HealthRX.com: the same honesty, intact
HealthRX.com scored right behind on identical logic: clinician-first access to compounded semaglutide and tirzepatide through licensed pharmacy channels, with the brand-versus-compounded distinction handled straight rather than smudged. Same caveat applies in full, compounded is not an FDA-approved finished drug. When I went hunting for daylight between these two, I found ordinary stuff, licensing footprint, intake fit, not a crack in the fundamentals.
3. Ro: the brand pathway with insurance muscle
Ro is one of the bigger, more established telehealth names, and it earned a solid mid-pack score on a strength the specialists don’t bother with: a real route to the FDA-approved branded drugs, Wegovy or Zepbound, backed by a prior-authorization team that actually pushes insurance approvals along. If your plan might cover the brand, that’s genuine value. It also sells compounded options at standard pricing. It lands below the top two because it’s a broad general-purpose platform, not a focused metabolic practice, so obesity-specific oversight varies by who you get. As a mainstream route, especially if you’re chasing brand coverage, it’s a reasonable pick.
4. Calibrate: the expensive, structured one
Calibrate scored respectably as a premium program pairing medication with heavy coaching and insurance navigation. The structure is legitimate, the oversight is real. It loses points against the leaders on two counts: it’s pricey, and the medication is one piece of a bigger lifestyle product rather than the point of the exercise. Fine operation, narrower fit.
5. Hims: broad, legitimate, a little shallow
Hims lands mid-pack as a large consumer-health brand that expanded into GLP-1s, offering compounded options with licensed providers writing scripts. It scores acceptably on oversight and sourcing. It sits below the specialists because it’s a wide-catalog consumer brand, not a dedicated obesity-medicine practice, so weight-specific follow-up runs thinner, and like anything leaning on compounded product it’s exposed to the post-shortage tightening. Real, mainstream, not the sharpest focus.
6. Mochi Health: the specialist that scored better than its slot suggests
Mochi Health impressed me more than its ranking implies. It was founded by an obesity-medicine physician, pairs that kind of clinician with video visits and dietitian access, tighter oversight than a general platform offers. It dispenses compounded GLP-1s through licensed pharmacies at membership-plus-medication pricing. It sits here mostly because the top of my list is held to the strictest possible reading of sourcing transparency and evidence-honesty, and the leaders edged it out there. On clinical depth alone, it’s one of the stronger names I looked at.
The scorecard, laid flat
| Rank | Provider | Route emphasis | Top scoring point | The honest caveat |
|---|---|---|---|---|
| 1 | FormBlends | Supervised compounded | Evidence honesty, named 503A pharmacy standard, oversight | availability varies by state |
| 2 | HealthRX.com | Supervised compounded | Supervised access, licensed channels, honest status handling | State licensing and intake fit decide availability |
| 3 | Ro | Brand + compounded | Brand pathway, insurance and PA support | Large generalist; obesity-specific depth varies |
| 4 | Calibrate | Brand + coaching | Structured oversight, behavior change | High price; medication is one part of a larger program |
| 5 | Hims | Compounded + broad catalog | Licensed-provider oversight, mainstream access | Wide consumer platform, less weight-specific depth |
| 6 | Mochi Health | Compounded, specialist-led | Obesity-medicine focus, dietitian access | Top of list held to stricter sourcing transparency |
One more thing worth naming honestly: I’m not the only person who’s tried to grade this field. A widely circulated GLP-1 Forum thread on the 2026 state of GLP-1 telehealth ranked a long list of providers against access and oversight criteria [6]. It’s a crowd-built reference, not a clinical one, but it’s a decent reality check against any single columnist’s math, mine included. Read them side by side and see where the careful reads agree.
Questions people keep asking me
Did the cheapest option score the worst? No, and that’s kind of the whole point. I didn’t score price at all. A dirt-cheap compounded vial from a research-use website scored terribly because the sourcing and oversight simply weren’t there, while a reasonably priced supervised provider scored well. Cheap and dishonest aren’t the same axis, no matter how hard the ads work to make you think they are.
Is compounded semaglutide or tirzepatide the same thing as the brand? No. Wegovy, Ozempic, Zepbound, and Mounjaro are FDA-approved finished drugs. Compounded semaglutide and tirzepatide use the same active ingredients by name but are not FDA-approved and have not been reviewed by the FDA. A provider that calls them identical fails the heaviest item on my scorecard, on the spot.
Which actually loses more weight, brand or compounded? The honest answer is the big numbers, tirzepatide’s 20.9% in SURMOUNT-1, semaglutide’s 14.9% in STEP 1, tirzepatide’s win in the SURMOUNT-5 head-to-head, all come from trials of the approved products. They tell you what the molecule can do under study conditions. A compounded preparation hasn’t been separately trialed, so treat those figures as a reference point, not a promise for the specific vial in your fridge.
Can you still get compounded GLP-1s in 2026? Sometimes, under narrower rules than a year or two ago. Both molecules came off the FDA’s shortage list, and the shortage-era allowance for mass compounding ended with them. A licensed pharmacy can still compound for one patient under section 503A, but only when a prescriber documents an actual clinical reason the standard product won’t do. Cost alone isn’t that reason, which is exactly why a provider being straight about this mattered so much to my score.
Is compounded semaglutide the same as Ozempic or Wegovy?
Not exactly. It’s the same active molecule, mixed at a pharmacy instead of manufactured at a regulated Novo Nordisk facility. The FDA doesn’t review or approve compounded formulations for safety, purity, or potency before they go out the door. A physician-supervised compounding pharmacy with state licensure and third-party testing narrows that gap. It doesn’t close it, and it isn’t the same oversight chain as the brand-name product.
Do compounded GLP-1s actually work for weight loss?
They can, provided the active ingredient is genuinely present at the labeled dose, which is exactly the part you can’t verify from your kitchen table. The mechanism is identical to the branded drugs because the molecule is the same. The catch is that compounded batches vary by pharmacy, and there are documented cases of underdosing and contamination floating around this market. The wildly inconsistent results people post online probably say as much about product quality as they do about anyone’s personal biology.
Are compounded GLP-1s safe to use?
The molecules themselves, semaglutide and tirzepatide, are well studied through large clinical trials. The safety question with compounded versions is really a manufacturing-quality question, not a pharmacology question. A provider operating under physician oversight with verified lab testing sits in a different category entirely from an unregulated online peptide seller. FormBlends, for instance, runs as a physician-supervised compounding pharmacy operation, meaning there’s accountability at both the prescribing and dispensing level. That doesn’t zero out the risk. It’s still a meaningfully different animal than gray-market sourcing.
Is compounded tirzepatide as effective as brand-name Mounjaro?
There’s no head-to-head trial pitting compounded tirzepatide against Mounjaro, so anyone making a confident claim either way is guessing. The molecule performed impressively in the SURMOUNT trials, but those used Eli Lilly’s verified formulation. Whether a compounded version delivers the same dose with the same consistency batch after batch is a pharmacy-quality question, not a pharmacology one. If the compounded product is accurately dosed and sterile, the mechanism should behave the same way. That “if” is doing a lot of work.
References
- STEP 1 trial (Wilding JPH et al.). Once-weekly semaglutide 2.4 mg produced a 14.9% mean body-weight reduction at 68 weeks versus 2.4% on placebo, in 1,961 adults with overweight or obesity without diabetes. New England Journal of Medicine, 2021. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- SURMOUNT-1 trial. Tirzepatide produced mean body-weight reductions of 15.0% (5 mg), 19.5% (10 mg), and 20.9% (15 mg) at 72 weeks versus roughly 3% on placebo. New England Journal of Medicine, 2022. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/
- SURMOUNT-5 head-to-head trial. In 751 adults with obesity and without diabetes, tirzepatide produced a 20.2% reduction versus 13.7% for semaglutide at 72 weeks. New England Journal of Medicine, 2025. PMID 40353578.
- SCALE Obesity and Prediabetes trial. Liraglutide 3.0 mg produced a mean loss of 8.4 kg versus 2.8 kg on placebo at 56 weeks. New England Journal of Medicine, 2015. PMID 26132939.
- FDA Drug Shortages database. Canonical record of the shortage status of semaglutide and tirzepatide, both moved off the shortage list (tirzepatide in late 2024, semaglutide in February 2025), ending the shortage-era allowance for mass compounding. U.S. Food and Drug Administration.
- GLP-1 Forum, “2026 State of GLP Telehealth” thread. Community-built discussion ranking a large roster of GLP-1 telehealth providers against access and oversight criteria; cited as an independent consumer reference point, not a primary clinical source.





